Join the ISFGS North American Chapter webinar on May 28th for a discussion on fluorescence-guided sentinel lymph node surgery and the evolving role of IC-Flow beyond conventional mapping techniques.
Featuring: Dr. Fernando Dip Dr. Alberto Rancati Moderator: Dr. Martin Newman
This session will explore how fluorescence-guided imaging is supporting surgical decision-making and advancing precision in surgical oncology.
Join the ISFGS North American Chapter for a focused session on fluorescence-guided pediatric surgery, exploring how real-time visualization can support safer and more precise decision-making in complex cases.
October 15th 7:00 PM EST Language: English
Speakers: Timothy B. Lautz, MD Seth D. Goldstein, MD, MPhil
Learn from leading experts in pediatric surgical oncology and thoracic surgery as they share clinical insights and practical applications of fluorescence imaging.
Título del video: Vessel Skeletonisation in Lateral Pelvic Lymph Node Dissection for Patients with Anomalous Anatomy after Neoadjuvant Treatment for Locally Advanced Rectal Cancer
Speakers: G Karagiannidis, MD, L Algazawi, MD, R Labinoti, MD, Arshad Malik, MD
Descripción: This video demonstrates vessel skeletonisation during lateral pelvic lymph node dissection in patients with complex or anomalous anatomy following neoadjuvant therapy for locally advanced rectal cancer. The technique highlights precise vascular dissection and careful anatomical identification to optimize oncologic outcomes while minimizing complications.
Descripción del evento: Join this North American Chapter session focused on bowel anastomosis in fluorescence-guided colorectal surgery, highlighting current techniques and clinical insights to optimize surgical outcomes.
Taking place on June 4th at 7:00 PM (EST), this session will be delivered in English and brings together leading experts in the field: Marylise Boutros, Patricia Sylla, and Steven D. Wexner.
An opportunity to deepen your understanding of fluorescence-guided approaches in colorectal surgery and learn from internationally recognized specialists.
Join this North American Chapter session focused on bowel anastomosis in fluorescence-guided colorectal surgery, highlighting current techniques and clinical insights to optimize surgical outcomes.
Taking place on June 4th at 7:00 PM (EST), this session will be delivered in English and brings together leading experts in the field: Marylise Boutros, Patricia Sylla, and Steven D. Wexner.
An opportunity to deepen your understanding of fluorescence-guided approaches in colorectal surgery and learn from internationally recognized specialists.
Indocyanine green (ICG) fluorescence imaging is increasingly used in colorectal resection to assess bowel perfusion and support safe anastomosis. In the EMEA region, optimized dosing and timing protocols help surgeons achieve consistent visualization of vascularization and reduce the risk of complications such as anastomotic leaks.
This approach enhances intraoperative decision-making by providing real-time feedback on tissue viability and perfusion.
Sección:
Tabla:
Columna1:
Region of interest
, Contenido:
Transection line
Columna1:
Dose
, Contenido:
5 mg bolus
Columna1:
Route
, Contenido:
I.V.*
Columna1:
Injection time
, Contenido:
Intraoperatively
Columna1:
First ICG detection
, Contenido:
10-60 sec
Columna1:
ICG Duration
, Contenido:
3 min
Columna1:
Camera requirements
, Contenido:
Laparoscope, NIR light source camera
Columna1:
References (full ref details at end of this guide doc)
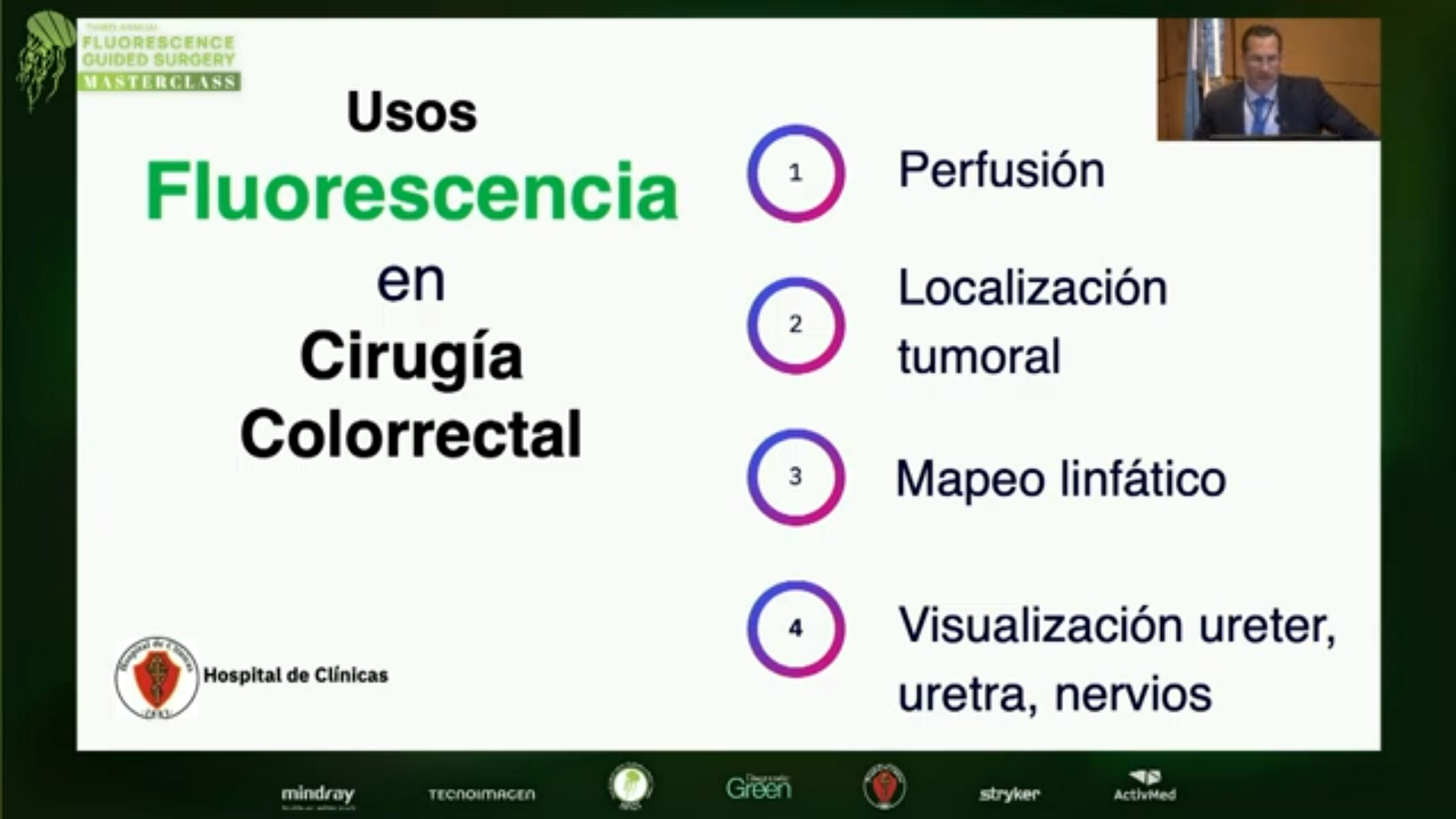
Indocyanine green (ICG) fluorescence imaging is increasingly used in colorectal cancer surgery to support both perfusion assessment and lymphatic mapping. This technique enables real-time visualization of tissue vascularization and lymphatic drainage, helping surgeons optimize resection margins and improve staging accuracy.
ICG-guided imaging has shown potential in identifying sentinel lymph nodes and detecting metastatic pathways, supporting more precise surgical planning while potentially reducing unnecessary lymphadenectomy.
In the EMEA region, standardized dosing and timing protocols help ensure consistent fluorescence imaging and enhance intraoperative decision-making in colorectal cancer procedures.
Indocyanine green (ICG) fluorescence imaging is increasingly used in complex procedures such as hysterectomy, colorectal, pelvic, and abdominal vascular surgery to enhance visualization of anatomy and assess tissue perfusion. This technique enables real-time identification of critical structures—including ureters, vessels, and lymphatics—supporting safer dissection and reducing the risk of intraoperative complications.
ICG fluorescence also supports evaluation of bowel and organ perfusion, helping surgeons optimize resection strategies and improve surgical precision in highly demanding procedures.
In the EMEA region, standardized dosing and timing protocols help ensure consistent fluorescence imaging and enhance intraoperative decision-making across multidisciplinary surgical settings.
Sección:
Tabla:
Columna1:
Region of interest
, Contenido:
Ureter localisation
Columna1:
Dose
, Contenido:
2.5 mg/mL
Columna1:
Route
, Contenido:
5 mL into each ureteric catheter
Columna1:
Injection time
, Contenido:
Prior to procedure
Columna1:
First ICG detection
, Contenido:
Beginning of surgery
Columna1:
ICG Duration
, Contenido:
Remains visible during procedure
Columna1:
Camera requirements
, Contenido:
Laparoscope, NIR light source camera
Columna1:
References (full ref details at end of this guide doc)
Indocyanine green (ICG) fluorescence imaging is increasingly used in colorectal and gastrointestinal cancer surgery to visualize lymphatic drainage and identify sentinel lymph nodes. When combined with near-infrared imaging systems, ICG enables real-time mapping of lymphatic pathways and supports more precise oncologic surgery.
This dosing chart outlines recommended ICG administration for colorectal and gastrointestinal carcinoma procedures, including peritumoral injection techniques, dosage per tumor quadrant, and timing of administration. These parameters help optimize sentinel lymph node detection and lymphatic mapping during fluorescence-guided surgery.
Dilution (25 mg in 10 mL of sterile water - 2.5mg/mL):
, Contenido:
Yes
Columna1:
Requires Flush with Sterile Water:
, Contenido:
No
Columna1:
Proposed Dosage:
, Contenido:
1 mL
Columna1:
Injection Time:
, Contenido:
Intraoperatively
Columna1:
First Indocyanine Green Detection:
, Contenido:
Minutes after administration
Columna1:
Indocyanine Green Duration:
, Contenido:
Stable during surgery. Slowly diffuses through lymphatics
Columna1:
Camera Requirements (handheld device, laparoscope or both):
, Contenido:
Both
Columna1:
Tips & Tricks:
, Contenido:
Intramural tumor: Intraoperative administration avoiding too much depth into the mucosa. Gastric lymphatics mapping: consider endoscopic peritumoral dye administration 24 hrs prior to lymphadenectomy.
Indocyanine green (ICG) fluorescence imaging is widely used in colorectal surgery to assess tissue perfusion and support safe intestinal dissection and anastomosis. By using near-infrared fluorescence imaging, surgeons can visualize real-time blood flow to the bowel and evaluate vascularization before performing colorectal anastomosis.
This dosing and timing chart provides guidance on recommended ICG administration for colorectal dissection procedures, including intravenous injection protocols, dosage ranges, and expected fluorescence detection times. These parameters help optimize intraoperative perfusion assessment and improve surgical decision-making during fluorescence-guided colorectal surgery.
Sección:
Title: Dosing & Timing Chart, Tabla:
Columna1:
Purpose:
, Contenido:
Perfusion assessment
Columna1:
Injection Type:
, Contenido:
Intravenous
Columna1:
Dilution (25 mg in 10 mL of sterile water - 2.5mg/mL):
, Contenido:
Yes
Columna1:
Requires Flush with Sterile Water:
, Contenido:
Yes
Columna1:
Proposed Dosage:
, Contenido:
3 mL
Columna1:
Injection Time:
, Contenido:
Intraoperatively
Columna1:
First Indocyanine Green Detection:
, Contenido:
30–60 seconds after administration
Columna1:
Indocyanine Green Duration:
, Contenido:
60 seconds–3 minutes
Columna1:
Camera Requirements (handheld device, laparoscope or both):
, Contenido:
Both
Columna1:
Tips & Tricks:
, Contenido:
Perform tissue vitality assessment as necessary prior to resection. Repeat assessment after anastomosis.
Indocyanine green (ICG) fluorescence imaging is increasingly used during abdominal and pelvic surgery to assist in ureter localization and help prevent inadvertent ureteral injury. With near-infrared fluorescence imaging, surgeons can visualize ureteral pathways in real time, improving anatomical identification during complex surgical procedures.
This dosing and timing chart provides guidance on recommended ICG administration techniques for ureter localization, including injection methods, dosage considerations, and expected fluorescence detection timing to support safe and effective fluorescence-guided surgery.
Sección:
Title: Dosing & Timing Chart, Tabla:
Columna1:
Purpose:
, Contenido:
Visualization of ureters
Columna1:
Injection Type:
, Contenido:
Other
Columna1:
Description:
, Contenido:
Cystoscopy guidance is recommended for retrograde intraureteral dye administration
Columna1:
Dilution (25 mg in 10 mL of sterile water - 2.5mg/mL):
, Contenido:
Yes
Columna1:
Requires Flush with Sterile Water:
, Contenido:
No
Columna1:
Proposed Dosage:
, Contenido:
5 mL per ureter
Columna1:
Injection Time:
, Contenido:
Prior to pelvic dissection
Columna1:
First Indocyanine Green Detection:
, Contenido:
During pelvic dissecction
Columna1:
Indocyanine Green Duration:
, Contenido:
Remains stable during surgery
Columna1:
Camera Requirements (handheld device, laparoscope or both):
, Contenido:
Both
Columna1:
Tips & Tricks:
, Contenido:
Advance ureteral catheter to ensure comprehensive assessment of the ureteral course